



Don't Miss Posterior Wall MIs
Because Minutes Mean Cardiac Muscle

Nearly everyone knows that a myocardial infarction with ST segment elevation (STEMI) is an emergency because the sooner the occluded coronary artery is opened, the better the prognosis. Such patients should undergo immediate percutaneous coronary angioplasty (PTCA) or thrombolytic therapy if the PTCA will be delayed more than 120 minutes. That’s because of 3M, no, not the company, but the rule that Minutes Mean (cardiac) Muscle. But emergency PTCA is often delayed in posterior wall MIs (PWMI), because PWMI’s are often not “seen” as a STEMI, at least not in the standard leads.
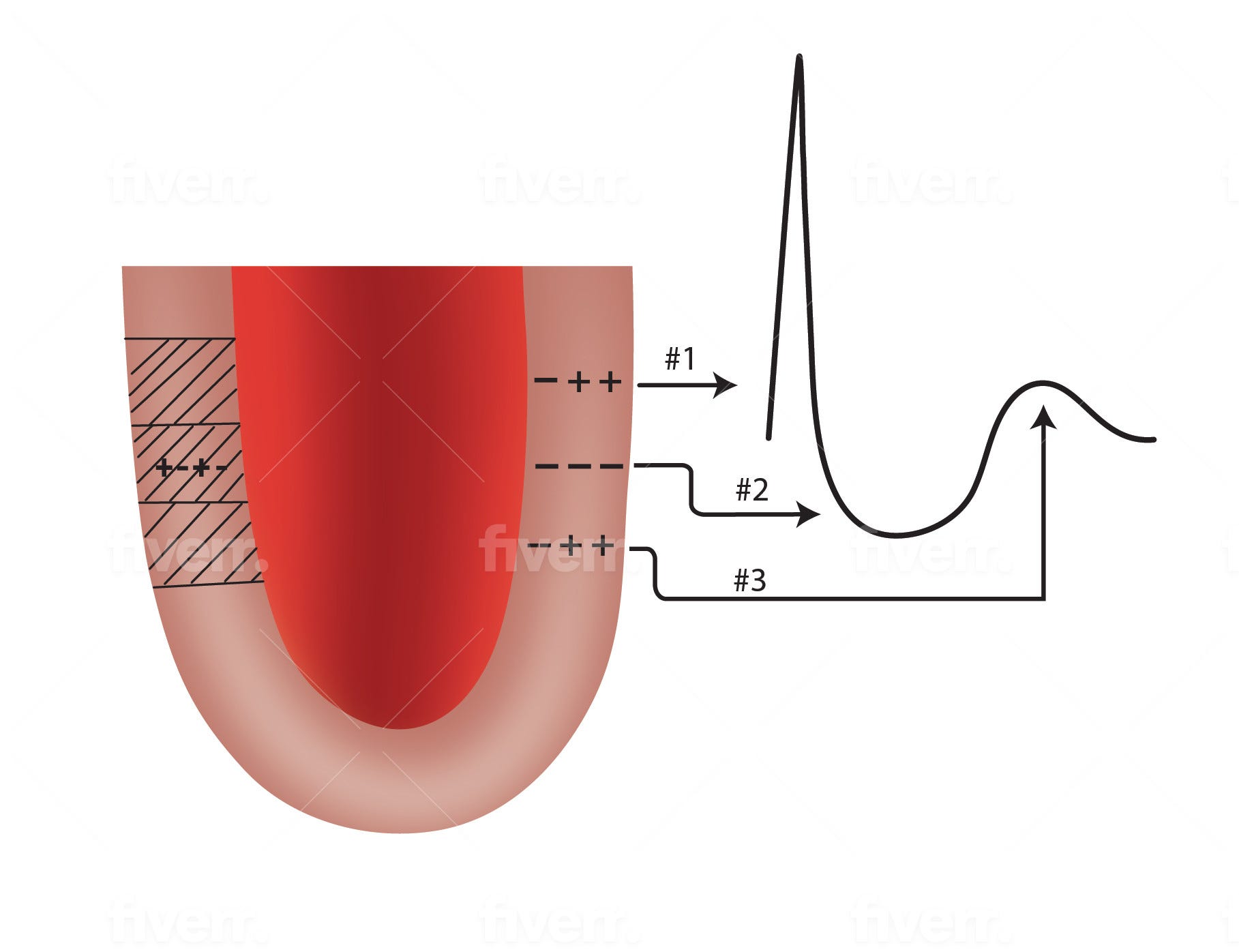
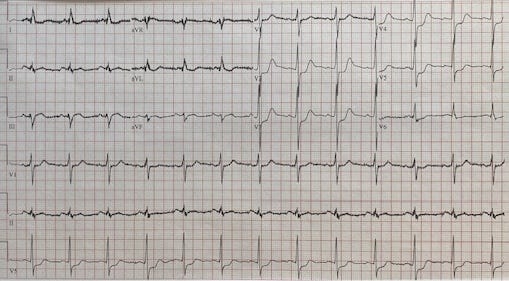
Three prior posts discussed normal myocardial depolarization/repolarization (1), R and T wave concordance (fancy word for going in the same direction)(2), and the window theory of q waves(3). But with PWMI, instead of a q wave in the anterior leads, the R wave in anterior leads V2 and V3 is taller than normal. The height of a non-infarct anterior R waves is normally decreased slightly because the posterior wall’s depolarization is going away from the anterior wall and its leads. If there is a PWMI, there is no competing electrical activity from the back wall so the anterior R wave is taller. Similarly, instead of ST elevation in the anterior leads there is ST depression. All of this is depicted graphically in the above figure with this post. The ECG included below shows a PWMI. You can see it easily if you print out the ECG, flip it over, and hold it up to the light. It looks just like an STEMI.
Many emergency department, internal medicine and cardiology clinicians do not know this. Often patients with PWMI are treated non-emergently because they had anterior ST segment depression. But this ST depression would be ST elevation if the leads were placed on the back along the bottom of the left scapula. Also, remember that the troponin may not be elevated initially if the sample is obtained soon after the start of the event, the vessel is totally occluded and the patient has not yet “flushed the toilet”.(4)
There are three rules here:
1. Symptoms overrule the electrocardiogram (ECG) which overrules the enzymes.
2. Never ignore a good story for an MI even if the ECG and troponins are initially normal. It takes time for the ECG to change, and sometimes the ECG never looks badly abnormal with PWMI. Why? Because the back wall of the heart is a long way from the precordial leads. Voltage decreases with distance so the abnormal voltage from the PWMI may not be obvious. And the troponin can be normal initially as mentioned above.
3. Doing a “flipping” ECG will help see the MI, especially if you flip the ECG and hold it up to the light.
References
1. https://pauldthompsonmd.substack.com/p/the-r-wave-and-t-wave-are-buddies
2. https://pauldthompsonmd.substack.com/p/i-hate-waiting-in-line
3. https://pauldthompsonmd.substack.com/p/how-do-myocardial-infarcts-create
4. https://pauldthompsonmd.substack.com/p/make-sure-the-patient-flushed-the
#cardiology #myocardial infarction #heart attack #electrocardiogram #troponin