



The R wave and T wave are Buddies
- And Generally Go Everywhere Together

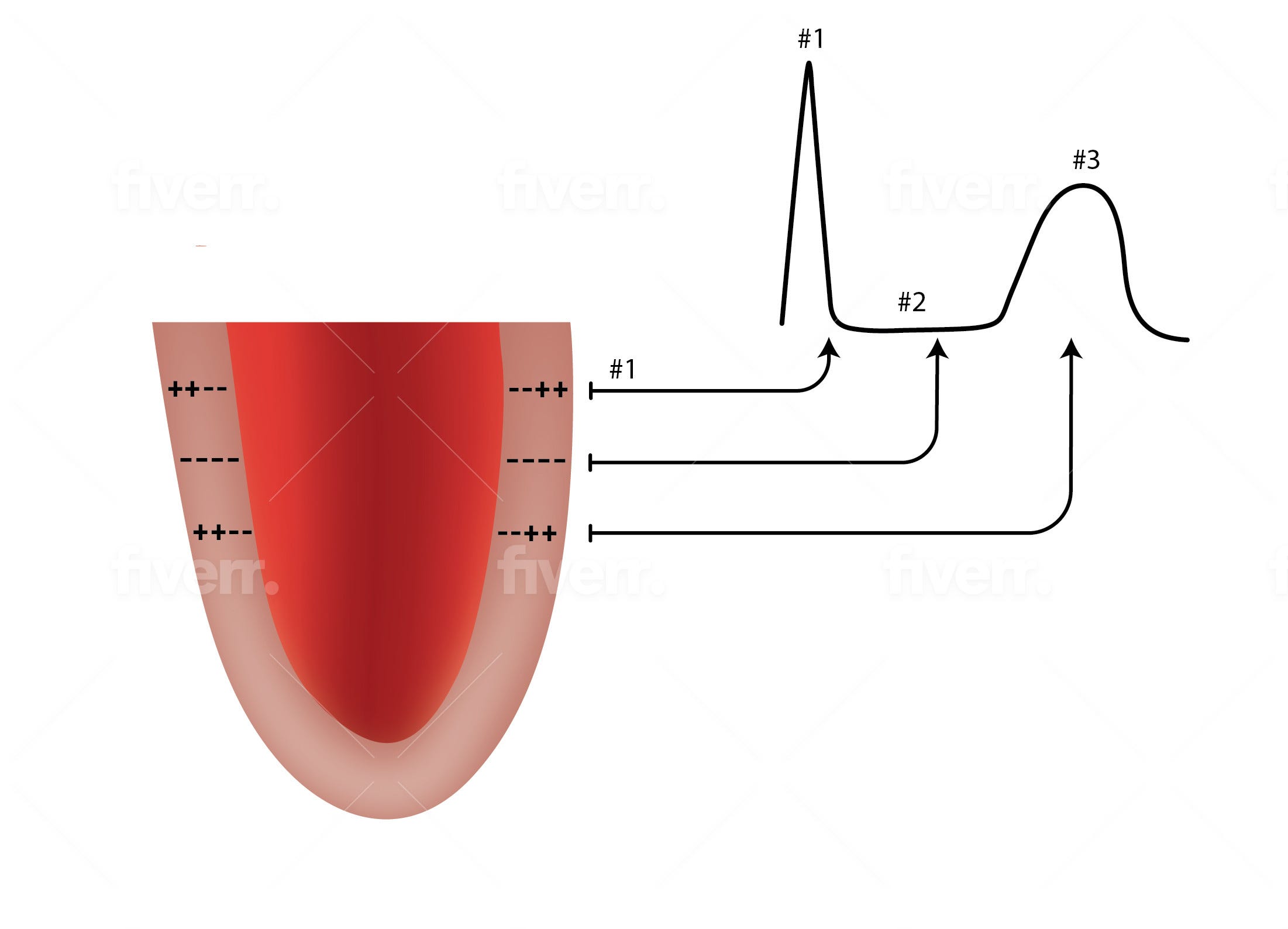
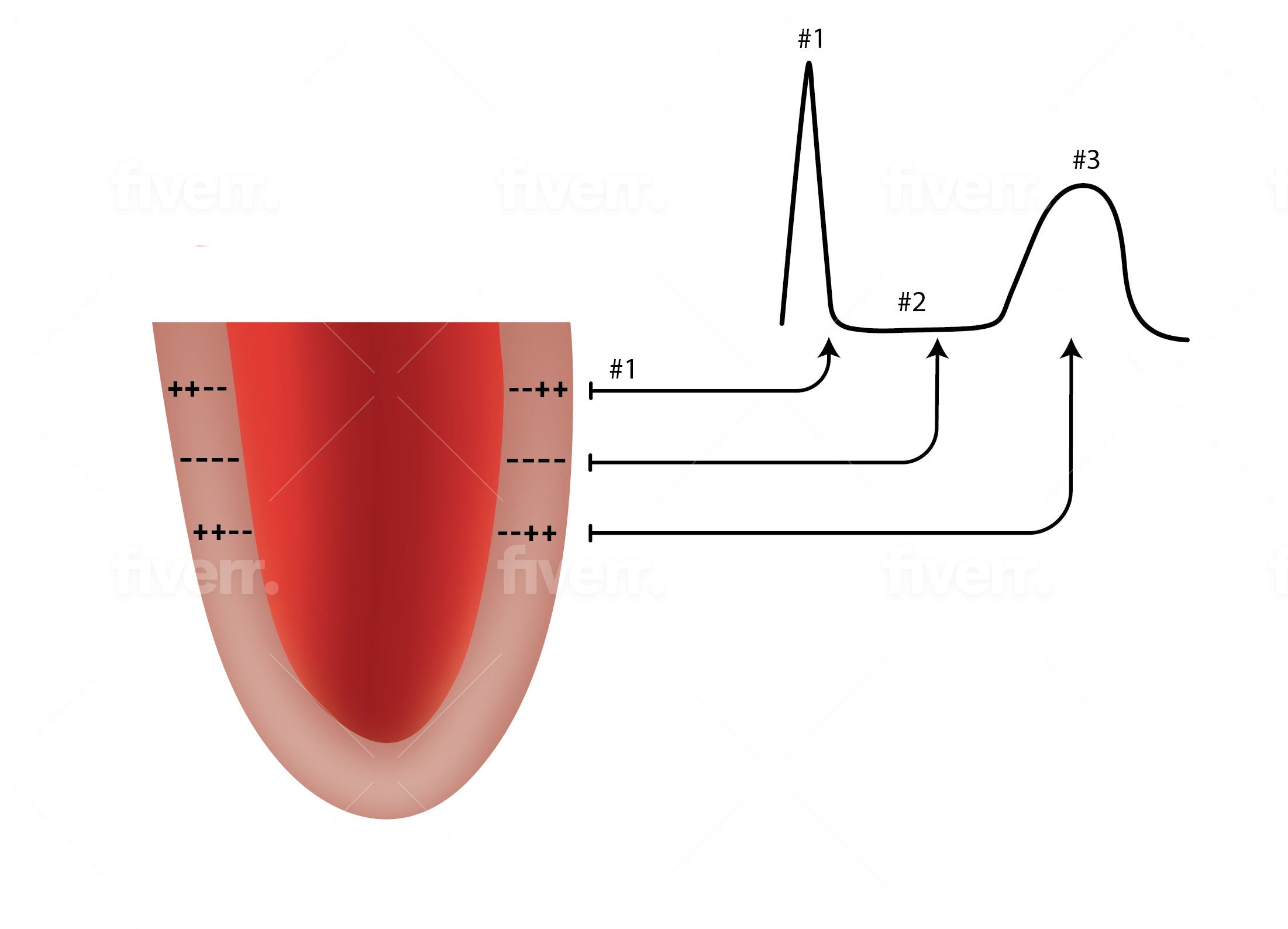
The heart muscle depolarizes from the inside (the endocardium) toward the outside (the epicardium). That means the inside goes from being electrically positive (+) to being electrically negative (-). Since vectors have positive heads or directions, this creates a positive vector over the depolarizing area. (See Figure) This positive deflection is the “R wave” of the ECG (#1 in the Figure) .
After depolarization there is a time of less electrical activity that occurs after the R wave. This is the ST segment (#2 in the Figure).
When the heart repolarizes, it does so in the opposite direction of depolarization. Specifically, the heart repolarizes (meaning the cells become + again) from the epicardium toward the endocardium. This creates the T wave (#3 in the Figure). But, even though the direction of repolarization is outside toward the inside, this creates a vector with a positive head, again pointed toward the epicardium. That means that the T wave is also upright, just like the R wave, because both vectors are directed toward the epicardium.
So, here’s the rule, one of the most important rules in cardiac electrophysiology: the R wave and the T wave in any lead of the ECG generally go in the same direction. They both should be positive or they both should be negative. In reality, the R and T wave vectors’ axes are not always exactly identical, but they are darn close. I remember that they should be “within 17 degrees of each other”, but cannot find a reference to prove that.
So, what does this mean clinically.
1. It means that surgery, anesthesiology, and the hospitalists should not put in a cardiac consult for “T-wave inversions in leads V1-V2”, if the R wave is also negative. This can also apply to lead V3. Getting concerned over a negative T wave in leads V1-2, and sometimes V3, is a very frequent cause of cardiology consults and sometimes surgery cancellations.
2. It also means that you should ignore the ECG computer’s reading of “possible anterior wall MI” when the only abnormalities on the ECG are T wave inversions with small R waves and even small Q waves (a negative wave) in V!-V2 and sometimes V3. When I discuss this with the team asking for the consult they say, “But it was read as a ‘possible MI’ by the cardiologist.” Nooooooo. ECGs are not read by cardiologists. They are read , by computers. They are reviewed by cardiologists for fun and profit. For cardiologists, the ECG machine makes the same “cha-ching” sound as a cash register, and the faster the ECGs are read the more frequent the cha-chinging. It takes a lot of time to change the “possible anterior wall MI” into “probably normal” so most ECG readers don’t take the time. And it is possible because anything is possible. Remember Mike Myers’ response in the 1992 movie Wayne’s World when he wished that he could do Wayne’s World for a living, “Yeah, and monkeys might fly out of my butt”.(1) Yeah, it is possible, but …. So, please do not over-react to the ECG if the T’s are down in the right precordial leads as long as the T and R go together and even if it’s been “read by a cardiologist”.
3. Finally, inversion of both the R and T waves in the limb leads 2, AVL and AVF where they don’t usually occur) in a person without heart disease should make you wonder if the limb leads are reversed. There are other things to look at as well, but consider this possibility first.
Remember that the R wave and T wave are buddies and that they normal go places together.
#cardiology #ECG #Twave #electrocardiogram #electrophysiology #cardiac rhyth
m