



Don’t Give False Reassurance
Measure Lipoprotein (a) Before Saying “Don’t Worry, Be Happy”

One of my interests is preventive cardiology, so I am often asked to see patients who are worried about their risk of heart disease because of a threatening family history. Sometimes their lipids are good and their hemoglobin A1C is normal, but before you tell them, “don’t worry, be happy” make sure you measure lipoprotein (a) [Lp(a)]. Patients with an elevated Lp(a) have an increased risk of heart disease even if their lipids are not excessively elevated.
I wrote previously that a ZERO coronary artery calcification (CAC) score is essentially a “ticket to ride” because the chance of an atherosclerotic cardiovascular event over the next 10 years is only ~2 to 4%.1 But we reported two women, aged 48 and 55, with angina and very tight LAD stenoses who had CAC scores of only 0 and 1.2 Both women had markedly elevated Lp(a) values of 477 and 314 n/mol, respectively. An optimal value is <75. So again, even with no or a low CAC, measure Lp(a) before you provide reassurance.
The rule: Don’t give reassurance with good lipid levels alone or with a CAC of zero alone; measure Lp(a) so you don’t give false reassurance.
So, what is Lp(a)? It's NOT apolipoprotein A. Apolipoprotein A is the major HDL apolipoprotein, so it’s a good guy/gal. Lp(a) is not in HDL and is a form of LDL cholesterol that markedly increases the risk of cardiovascular disease. I mention the difference between Lp(a) and lipoprotein A because sometimes, when I have asked for an Lp(a), also called “lipoprotein little a”, someone orders an apolipoprotein A.
How does Lp(a) increase heart disease risk? No one knows for sure, but there are three possibilities (Figure)3
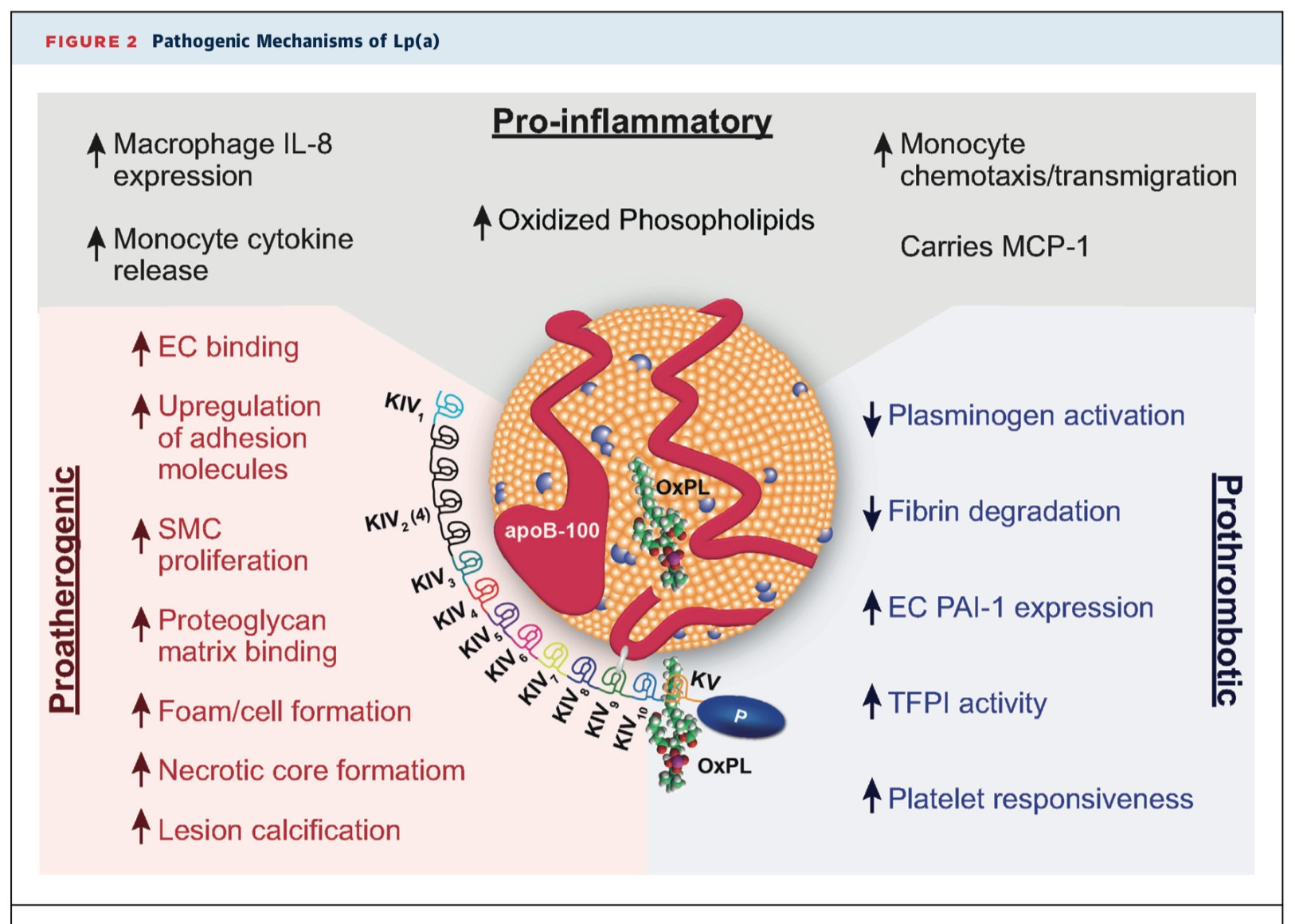
Reproduced from 3
1. Lp(a) contains a lot of phospholipid, which is inflammatory, so maybe it’s via inflammation.
2. Lp(a) contains cholesterol which could contribute cholesterol to the atherosclerotic plaque.
3. Part of Lp(a) has the same protein structure as plasminogen so it’s possible that Lp(a) interferes with plasminogen becoming plasmin. Plasmin dissolves blood clots, so if you make less plasmin, you are less able to dissolve that coronary thrombosis. Interestingly, Lp(a) might be a risk factor for strokes in the young. (4)
Many clinicians have not heard of Lp(a), but you will. It was first described in 1964, but is now all the rage. When some risk factor becomes “the rage”, it usually means that some company wants to make money by testing for it or treating it, and several companies are developing mRNA interference strategies to reduce it. We published a report way back in 1997 from one of our anabolic steroid studies that testosterone reduces Lp(a)4, but estrogen, niacin, thyroid, and proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors lower it, but all not too much.
The present approach to Lp(a)’s management is to lower the LDL as much as possible. This is the principle that when you can’t lower the risk factor, lower the risk, or when you cannot lower the Lp(a), lower the LDL with statins because statins clearly lower the risk. Most experts also suggest that individuals with elevated Lp(a) should take aspirin in part because in the ASPREE (ASPirin in Reducing Events in the Elderly) trial subjects with genotypes associated with elevated Lp(a) had fewer cardiovascular events.6
Wow, lots of stuff to remember. Here are the Rules:
1. Reassurance is a great treatment. Use it.
2. But don’t give reassurance that a patient has low cardiac risk before you measure Lp(a).
3. Don’t assume the patient is safe from atherosclerotic disease just because the lipids are good and the A1C is normal.
4. Don’t confuse lipoprotein (a) with apolipoprotein A.
5. Don’t assume a zero CAC score is a “ticket to ride” before you measure Lp(a).
6. If the Lp(a) is high, treat the risk because you can’t yet treat the risk factor.
1. https://pauldthompsonmd.substack.com/p/you-got-a-ticket-to-ride?utm_source=profile&utm_medium=reader2 (Accessed March 1, 20024
2. Haxhi J, Pershwitz G, Thompson PD. Coronary artery disease with normal lipids and low coronary artery calcium in two women with high lipoprotein(a). J Clin Lipidol. 2020 Mar-Apr;14(2):186-188. PMID: 31983675
3. Tsimikas S. A Test in Context: Lipoprotein(a): Diagnosis, Prognosis, Controversies, and Emerging Therapies. J Am Coll Cardiol. 2017 Feb 14;69(6):692-711. PMID: 28183512
4. https://www.ncbi.nlm.nih.gov/books/NBK395570/#:~:text=In%20adults%2C%20Lp(a),arterial%20ischemic%20stroke%20(AIS). (Accessed March 1, 2024)
5. Zmunda JM, Thompson PD, Dickenson R, Bausserman LL. Testosterone decreases lipoprotein(a) in men. Am J Cardiol. 1996 Jun 1;77(14):1244-7. PMID: 8651107
6. Aspirin for Primary Prevention of Cardiovascular Events in Relation to Lipoprotein(a) Genotypes.
7. Lacaze P, Bakshi A, Riaz M, et. al. Am Coll Cardiol. Aspirin for Primary Prevention of Cardiovascular Events in Relation to Lipoprotein(a) Genotypes. 2022 Oct 4;80(14):1287-1298. PMID: 36175048
This is a lovely breakdown. Thanks for writing these, Dr. Thompson.
Great information as always!