



#1 - Knowing What to Expect from an Anterior versus Inferior Wall Myocardial Infarction
Hypotension Has Different Causses and Treatments in Anterior vs Inferior MIs

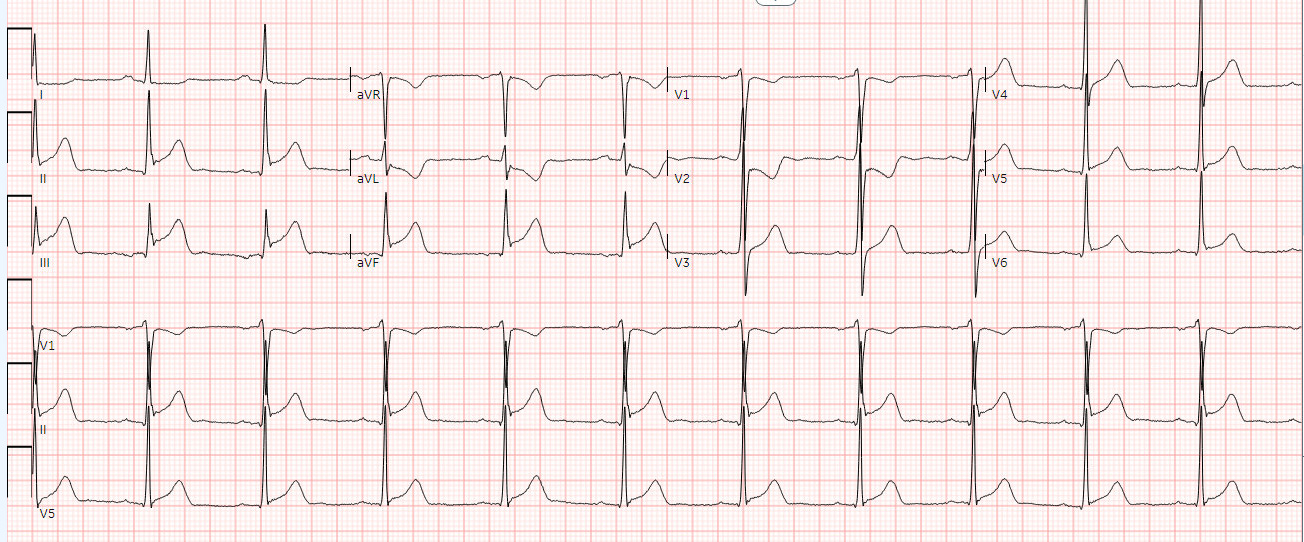
An Acute Inferior Wall MI
Present day clinicians rarely get to observe the clinical differences between anterior (AWMI) and inferior wall myocardial infarctions (IMI). This is because most patients are now treated promptly with thrombolytic therapy or acute angioplasty so that infarcts are not allowed to run their clinical course. Nevertheless, it’s important to know the differences in the clinical presentation so that clinicians can look for other causes if the clinical course does not proceed as expected. These differences are often not apparent when a patient presents early and promptly undergoes angioplasty, but these differences do appear in patients who present later in the course of the infarct. I am going to do several posts on the key differences between inferior and anterior wall MIs. This will be simple for some of you, but hopefully will include something novel even for the MI experts.
Patients with both IMI and AWMI often have systolic hypotension, but the causes are different. Approximately 30% of patients with IMI have a right ventricle (RV) infarction (RVI). The RV has thinner walls making it more responsive to intravascular volume than the left ventricle (LV). Infarction of the RV reduces RV stroke volume, which subsequently reduces LV stroke volume producing systemic hypotension. This can be treated by volume expansion using 2-4 liters of saline to fill the RV. The RV responds because it is very volume responsive. This volume responsiveness is also why patients with IMIs may become markedly hypotensive when given veno-dilating agents such as nitroglycerin or morphine.
In contrast, the hypotension produced by AWMI is caused by LV systolic dysfunction. Very small amounts of fluid can be administered in AWMI, but cautiously, because this rarely works in AWMIs and because the fluid leads to pulmonary edema. Hypotension in AWMIs is better treated with pressors if small amounts of fluid don’t work.
It is critically important not to give more than about 4 L of normal saline in IMIs because too much fluid can cause “pseudo tamponade”. The 4 L is totally arbitrary on my part, but provided as a reference of when enough is enough. Pressors are the next step, if the patient remains hypotensive after that amount of volume. Why is too much fluid a problem? Too much fluid can over fill the distensible RV, which can expand up against the pericardium producing “pericardial constraint”. If pericardial fluid accumulates slowly or the RV enlarges slowly, pericardial constraint is not a problem because the pericardium stretches. This is similar to the observation that tamponade can occur with small amounts of intrapericardial fluid if that fluid accumulates rapidly whereas effusions in cancer patients, for example, can be quite large without tamponade because they accumulate slowly and the pericardium stretches. In contrast, rapid expansion of the RV from the dilatation caused by the IMI plus too much intravascular fluid does not allow the pericardium to stretch. The enlarged RV and pericardial constraint reduces LV filling and produces tamponade-like physiology. That’s because with pericardial constraint, the heart is essentially “boxed in”. Any increase in the RV size decreases space for the LV and decreases LV filling and stroke volume. This “pseudo-tamponade” is often seen in IMI patients transferred to tertiary care facilities after over-zealous fluid replacement at outside institutions.
There was a paper published on this when I was a fellow in the early 1970’s, but I cannot find it. It was before echocardiography was available. My memory is that the authors attempted pericardiocentesis in seven patients with IMI who developed clinical findings of tamponade after aggressive fluid treatment of hypotension.
#myocardialinfarction #infarction #heartattack #pericardium #tamponade #pseudotamponade
This is great Dr. Thompson. plus I have learned from your previous posts that fluids can cause a fib as well.